These tumours arise throughout the body but the gastro-intestinal tract (especially the appendix and rectum), followed by the lung (bronchus), are the commonest sites.
The frequency in these sites reflects the relatively large number of neuro-endocrine cells normally found there. Similarly, in the pancreas, which is another common site for neuro-endocrine tumours (NETs), are commoner in the tail than the head because the Islets of Langerhans are present in a higher density in the tail.
NETs were previously called carcinoid tumours but now the term neuro-endocrine tumours is now preferred except in the lung where the original term is still used.
NETs are graded (1-3) according to their rate of proliferation of the tumour cells which can be assessed either by counting mitoses or using an immunohistochemical marker (Ki-67). The higher the rate, the higher the grade and the greater the risk of metastatic disease although there is no clear cut-off level. The tumours in the appendix and rectum almost always never metastasize. Small intestinal NETs are especially likely to do so. Challengingly the secondary tumours may be larger than the primary they arise from which can make it difficult to identify the latter.
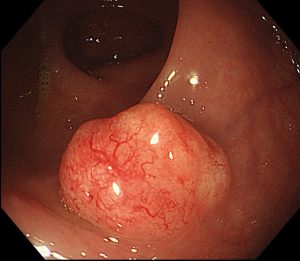
In the gastro-intestinal tract the tumours are usually submucosal although they may ulcerate. They may invade through the wall and may reach the peritoneal surface. They are often associated with a marked desmoplastic reaction. Multiple tumours may be seen; in the ileum 40% are multiple. Spread is to regional lymph nodes and the liver.
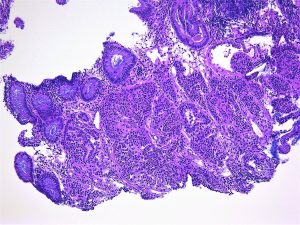
Histologically, NETS, are composed of relatively uniform cells arranged, in cords or nests, and have granular cytoplasm. The granules contain a protein, chromogranin, which can be used as an immunohistochemical or serum marker for these tumours.
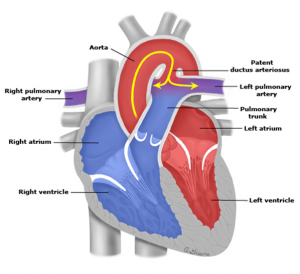
NETs may secrete a wide range of hormones. The carcinoid syndrome is associated with the secretion of serotonin usually by git tumours. It is characterized by diarrhoea and bronchospasm and may be associated with fibrosis involving the right-hand side of the heart which can produce distortion of the valves. It is only seen in tumours which have spread to the liver as otherwise the serotonin is broken down in the liver.
Below is are images of a rectal carcinoid tumour (made available by the excellent @Patholwalker).