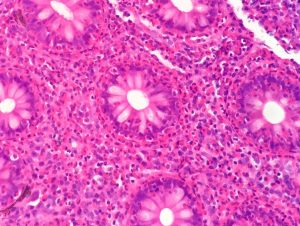
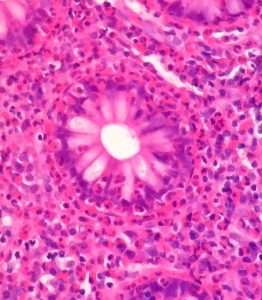
This post was stimulated by a case of eosinophilic colitis I reviewed at an MDT this morning. The images are below.
They show sheets of eosinophils in the lamina propria and infiltrating crypts. They are easily recognised by their bilobed nuclei and prominent red granules.
This was an opportunity to review eosinophils.
Eosinophils are conspicuous in inflammatory reactions triggered by IgE, such as asthma, and by parasites and are increased by TH-2 activation. IL-5 and GM-CSF increase the production of eosinophils by the bone marrow. They are associated are recruited into the tissue by eotaxins which are CC chemokines.
Eosinophils have 2 types of effector function:
- they release toxic granule proteins (e.g. major basic protein which is toxic to parasites) and free radicals.
- they synthesise prostaglandins, leukotrienes and cytokines.
In the context of this case, likely causes include gut parasites, such as schistosomiasis, and allergic reactions to drugs.
If you want to read more try the excellent British Society of Immunology Website: https://www.immunology.org/public-information/bitesized-immunology/cells/eosinophils
