Amputations are an important and largely preventable complication of type 2 diabetes mellitus that impact considerably on the life expectancy and quality of life of those affected. In England, more than 9000 diabetes-related amputations are performed each year, with decreasing rates but higher absolute numbers of major amputations, and the annual direct healthcare costs of diabetic foot ulceration and amputation are approximately £1 billion.
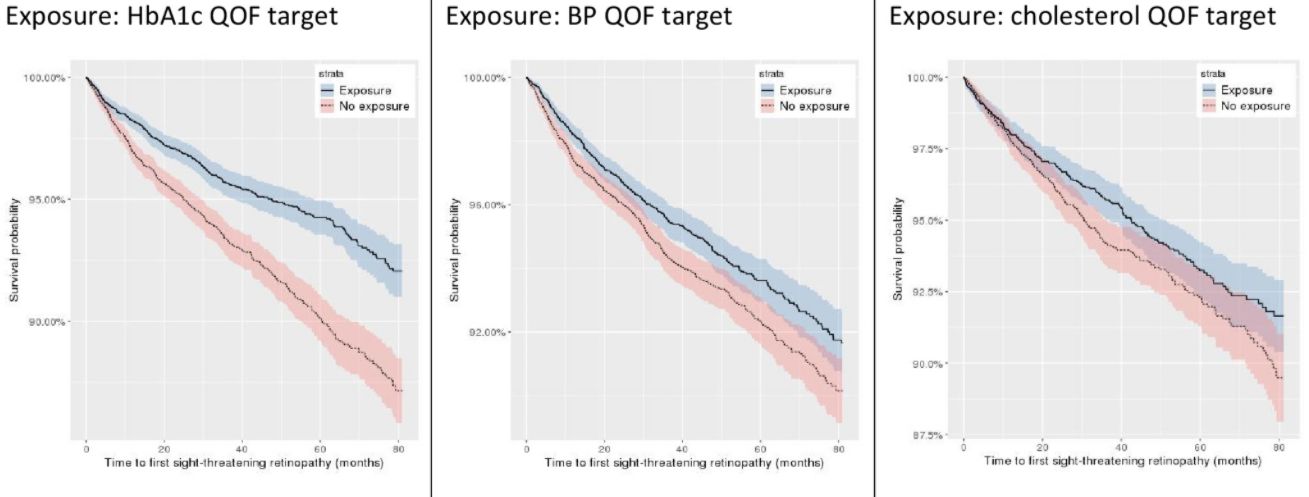
In an article published in BMJ Open Diabetes Research & Care, we investigated the associations between attainment of primary care quality clinical indicators, completion of National Diabetes Audit care processes, and non-traumatic lower limb amputations among people with type 2 diabetes. We observed that minor or major, as well as major-only, amputation rates were 26%–51% and 3%–51%, respectively, lower among those who met the HbA1c indicator and 14%–47% lower among those who met the cholesterol indicator for our primary outcome.
Comprehensive primary care-based secondary prevention may offer considerable protection against diabetes-related amputation. This has important implications for diabetes management and medical decision-making for patients, as well as type 2 diabetes quality improvement programs.
DOI: http://dx.doi.org/10.1136/bmjdrc-2020-002069
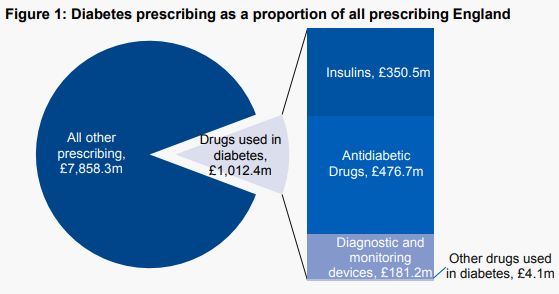 Drugs used to treat diabetes are now responsible for 11.4% of total primary care prescribing costs in England, £1,012 million annually. The very high costs to the NHS of treating diabetes are an inevitable consequence of the increase in the prevalence of type 2 diabetes in recent decades. This increase in the prevalence of type 2 diabetes is in turn a consequence of lifestyle factors such as high-calorie diets (particularly diets high in sugars and refined carbohydrates), physical inactivity and obesity. We need effective strategies at both population and individual level, and changes in the obesogenic environment we live in, to reverse these adverse lifestyle- associated factors and bring down the prevalence of type 2 diabetes.
Drugs used to treat diabetes are now responsible for 11.4% of total primary care prescribing costs in England, £1,012 million annually. The very high costs to the NHS of treating diabetes are an inevitable consequence of the increase in the prevalence of type 2 diabetes in recent decades. This increase in the prevalence of type 2 diabetes is in turn a consequence of lifestyle factors such as high-calorie diets (particularly diets high in sugars and refined carbohydrates), physical inactivity and obesity. We need effective strategies at both population and individual level, and changes in the obesogenic environment we live in, to reverse these adverse lifestyle- associated factors and bring down the prevalence of type 2 diabetes.